Tirzepatide
Summary
Tirzepatide is a synthetic 39-amino-acid peptide and the first dual GIP/GLP-1 receptor agonist ("twincretin"). Approved as Mounjaro for type 2 diabetes and Zepbound for weight management, it is dosed once weekly and is widely studied for glucose control and substantial weight reduction.
Quick facts
| Also known as | LY3298176, Mounjaro, Zepbound |
| Category | Metabolic — dual incretin (GIP/GLP-1) agonist |
| Status | FDA-approved (Mounjaro 2022; Zepbound 2023); active research compound |
| CAS | 2023788-19-2 |
| Formula | C225H348N48O68 |
| Molecular weight | 4813.5 g/mol |
| Sequence | 39-residue synthetic peptide; Aib at positions 2 and 13; C20 fatty-diacid acylation at Lys20 |
| Half-life | ~5 days (≈117 h) — supports once-weekly dosing |
| Storage | Lyophilized: cold, dry, dark. Reconstituted: refrigerate 2–8 °C, protect from light, use promptly. |
In Plain English
Tirzepatide is a peptide that copies two natural gut hormones that control appetite and blood sugar. It is the active ingredient in approved diabetes and weight-loss medicines and produces large weight loss in trials. Researchers and doctors study it for diabetes and obesity.
Tirzepatide is a once-weekly synthetic peptide first cleared as Mounjaro (2022) for type 2 diabetes and later as Zepbound (2023) for chronic weight management. It is widely discussed as the first “twincretin” — a single molecule engineered to switch on two gut-hormone receptors at once.
What is tirzepatide?
Tirzepatide (development code LY3298176; brand names Mounjaro and Zepbound) is a 39‑amino‑acid synthetic peptide developed by Eli Lilly. Its backbone is based on the native incretin hormone GIP, modified with a C20 fatty‑diacid chain that binds to albumin in the bloodstream and a pair of aminoisobutyric‑acid (Aib) substitutions that resist enzymatic breakdown. Together these changes give it a half‑life of roughly five days, which is what makes once‑weekly dosing possible.
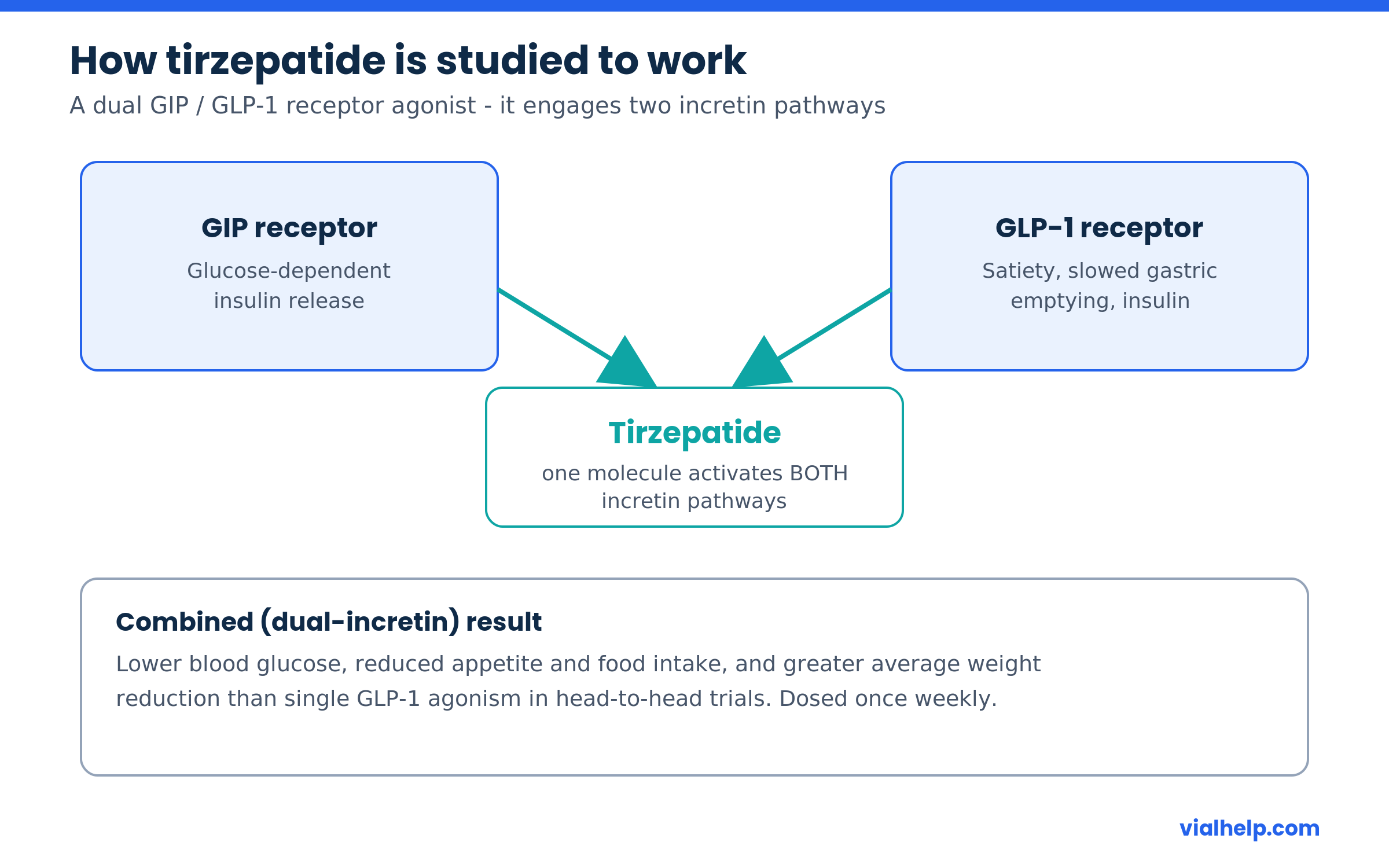
What sets tirzepatide apart from earlier incretin mimetics is that it is a dual agonist: it activates both the glucose‑dependent insulinotropic polypeptide (GIP) receptor and the glucagon‑like peptide‑1 (GLP‑1) receptor. Single‑target GLP‑1 drugs such as semaglutide engage only one of these pathways.
How tirzepatide is studied to work
Incretins are hormones the gut releases after eating; they prompt the pancreas to release insulin and signal the brain that you are full. Tirzepatide mimics two of these signals simultaneously. Researchers describe its activity through several converging pathways:
- GLP‑1 receptor activation — promotes glucose‑dependent insulin secretion, suppresses glucagon, and slows gastric emptying.
- GIP receptor activation — adds a second insulinotropic signal and is thought to influence fat metabolism and appetite centers.
- Central appetite signaling — both receptors are expressed in brain regions that regulate hunger and satiety, which is associated with reduced food intake.
- Glucose‑dependent action — because insulin release is tied to blood‑glucose levels, the mechanism carries a lower intrinsic hypoglycemia risk than fixed‑dose insulin.
Reported effects and benefits in the research literature
Across the clinical-development programs, tirzepatide has been associated with:
- Substantial reductions in HbA1c (blood‑sugar control) in type 2 diabetes trials.
- Large average body‑weight reductions — among the highest reported for an incretin therapy.
- Improvements in markers such as fasting glucose, blood pressure and lipid measures in trial populations.
- Approval data supporting use in obstructive sleep apnea linked to obesity.
What this does not mean: these are population‑level trial results reported under medical supervision with structured dose escalation. They are not a promise of individual outcomes, and they say nothing about unsupervised or research‑only use. Effects, tolerability and risks vary by person.
What the human evidence shows
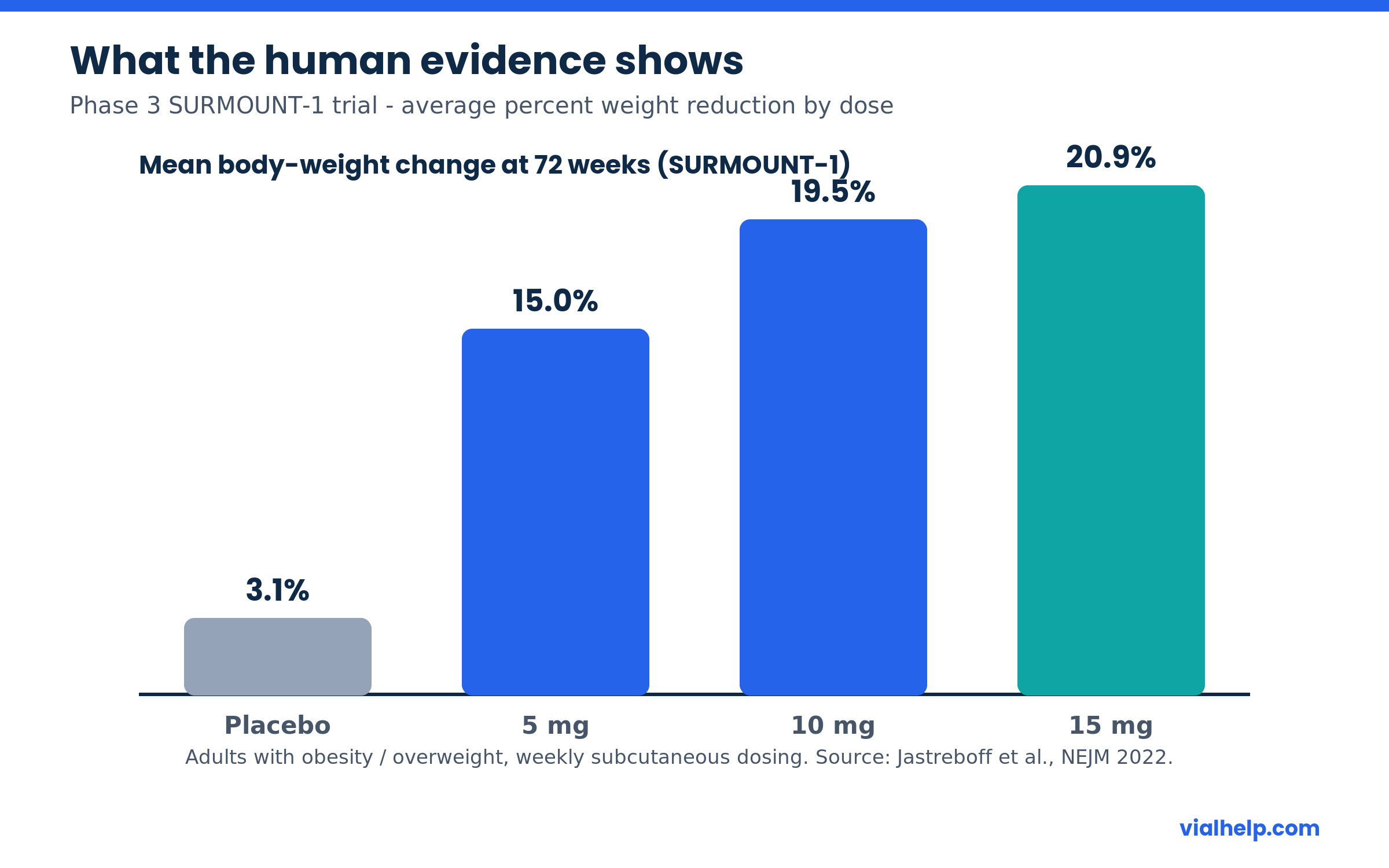
Tirzepatide is one of the most extensively trialed incretin peptides. In the SURPASS program (type 2 diabetes), it produced clinically meaningful HbA1c and weight reductions, and in the head‑to‑head SURPASS‑2 trial it outperformed semaglutide 1 mg on glucose control. In the SURMOUNT obesity program, SURMOUNT‑1 reported mean weight reductions of about 15%, 19.5% and 20.9% at the 5, 10 and 15 mg doses over 72 weeks, versus 3.1% with placebo.
On the regulatory side, the FDA approved Mounjaro for type 2 diabetes in May 2022, Zepbound for chronic weight management in November 2023, and later extended Zepbound to moderate‑to‑severe obstructive sleep apnea in adults with obesity. Both brands contain the same molecule; the names reflect different approved uses.
Handling, storage and reconstitution (research context)
- Lyophilized powder: keep cold and dry, protected from light, until reconstituted.
- Reconstituted solution: refrigerate at 2–8 °C, minimize light and agitation, and discard if cloudy or discolored.
- Add diluent slowly down the vial wall and swirl gently — do not shake, which can denature peptides.
- Always work out concentration before measuring. Our reconstitution calculator converts vial mg and diluent volume into mg/mL, and the IU vs mL explainer shows why a syringe “unit” is a volume mark, not a dose.
Cautions and considerations
- Tirzepatide sold as a “research compound” is not a quality‑controlled pharmaceutical; identity and purity should be verified against a Certificate of Analysis.
- It is a prescription medicine in approved settings; this page is informational and not a recommendation to obtain or self‑administer it.
- Gastrointestinal effects (nausea, diarrhea, vomiting, constipation) are the most commonly reported adverse events — see our companion article on GLP‑1 side effects.
- Informational use only — not medical advice. Consult a qualified healthcare professional. 21+.
Frequently asked questions
Is tirzepatide the same as semaglutide?
No. Both are incretin peptides, but semaglutide targets only the GLP‑1 receptor, while tirzepatide is a dual GIP/GLP‑1 agonist. In the SURPASS‑2 trial tirzepatide showed greater glucose lowering than semaglutide 1 mg.
What is the difference between Mounjaro and Zepbound?
They are the same molecule (tirzepatide) marketed under different names for different FDA‑approved uses: Mounjaro for type 2 diabetes and Zepbound for chronic weight management and obstructive sleep apnea.
Why is tirzepatide dosed only once a week?
A C20 fatty‑diacid chain lets the molecule bind albumin and circulate far longer than a natural incretin, giving it a half‑life of roughly five days — long enough for weekly dosing.
How is tirzepatide stored after reconstitution?
Reconstituted peptide is generally refrigerated at 2–8 °C, protected from light, and used promptly. See our storage and stability guide for general principles.
Related compounds and further reading
- Semaglutide — the single‑target GLP‑1 agonist most often compared with tirzepatide.
- How to reconstitute peptides
- Sterile technique
- Browse the full peptide library · All guides
- IU vs mL: why units are not a dose
Share this article
References
- Tirzepatide
- Jastreboff AM et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1), NEJM 2022
- Frias JP et al. Tirzepatide versus Semaglutide Once Weekly (SURPASS-2), NEJM 2021
- FDA Approves Lilly’s Zepbound (tirzepatide) for Chronic Weight Management
- DrugBank: Tirzepatide (DB15171)
- Tirzepatide – Wikipedia
For informational use only. Not medical advice; consult a qualified healthcare professional. 21+.
Tirzepatide reconstitution calculator
Use the calculator below to find the concentration (mg/mL), draw volume and U-100 syringe units for Tirzepatide once it is reconstituted with bacteriostatic water. Tirzepatide has molecular formula C225H348N48O68 and a molecular weight of 4813.5 g/mol. Enter your vial amount and the water volume to see the lab math — informational use only, not dosing advice.