Oxytocin
Summary
Oxytocin is a nine-amino-acid hormone made in the hypothalamus and released by the posterior pituitary, where it drives uterine contraction during labor and milk ejection during nursing. First synthesized by Vincent du Vigneaud in 1953 (the first polypeptide hormone ever made in the lab), it acts through a single oxytocin receptor. Beyond reproduction it is heavily studied for roles in social bonding, trust and stress, though human behavioral findings remain mixed. Informational only, not medical advice.
Quick facts
| Also known as | OXT, oxytocin acetate, Pitocin (synthetic), Syntocinon, alpha-hypophamine |
| Category | Neurohypophysial hormone / cyclic nonapeptide |
| Status | FDA-approved drug as synthetic oxytocin (Pitocin/Syntocinon) for labor induction/augmentation and postpartum hemorrhage; widely studied (e.g. intranasal) for social-behavioral research |
| CAS | 50-56-6 |
| Formula | C43H66N12O12S2 |
| Molecular weight | 1007.19 g/mol |
| Sequence | Cys-Tyr-Ile-Gln-Asn-Cys-Pro-Leu-Gly-NH2, disulfide bridge Cys1-Cys6 (PubChem CID 439302) |
| Half-life | Short — roughly 1-6 minutes in plasma (often cited ~3-5 min); rapid enzymatic clearance |
| Storage | Lyophilized: sealed, light-protected at -20 C or below. Reconstituted: refrigerate 2-8 C, protect from light, use within a short window; do not freeze-thaw. |
In Plain English
Oxytocin is a natural hormone the body makes that is involved in bonding, trust, and childbirth. A lab-made version is an approved medicine used during labor. Researchers also study it for social behavior and mood.
Oxytocin is one of the most-studied hormones in biology — a small, ring-shaped peptide that the body uses to coordinate childbirth, breastfeeding, and, possibly, the way mammals bond with one another. It was first isolated from posterior pituitary extracts in the early twentieth century, and in 1953 the American biochemist Vincent du Vigneaud determined its sequence and chemically synthesized it, making oxytocin the first polypeptide hormone ever built in a laboratory. That achievement earned him the 1955 Nobel Prize in Chemistry. Today oxytocin sits at the intersection of obstetrics, neuroscience, and behavioral psychology, and its name appears in everything from FDA drug labels to popular articles about the so-called “love hormone.”
What is Oxytocin?
Oxytocin (OXT, CAS 50-56-6) is a cyclic nonapeptide — nine amino acids in the sequence Cys-Tyr-Ile-Gln-Asn-Cys-Pro-Leu-Gly-NH2. A disulfide bridge links the two cysteine residues, folding the molecule into a six-residue ring with a short three-residue tail that ends in an amide group. Its molecular formula is C43H66N12O12S2 and its molecular weight is about 1007 g/mol (PubChem CID 439302). Structurally it is nearly identical to vasopressin (antidiuretic hormone), differing by only two amino acids, which is why the two hormones share overlapping receptor activity and a common evolutionary origin.
In the body, oxytocin is produced mainly by magnocellular neurons in the supraoptic and paraventricular nuclei of the hypothalamus. These cells transport the hormone down their axons to the posterior pituitary, where it is stored and released into the bloodstream. The same neurons, and a smaller parvocellular population, also project oxytocin within the brain itself, which is the basis for its proposed central, behavioral roles. The synthetic drug version — chemically identical to the natural hormone — is sold under names such as Pitocin and Syntocinon.
How Oxytocin is studied to work
Oxytocin acts through a single, well-characterized target: the oxytocin receptor (OXTR), a G-protein-coupled receptor. When oxytocin binds, the receptor couples mainly to Gq proteins and activates the phospholipase C pathway, generating inositol trisphosphate and releasing calcium from intracellular stores. In smooth muscle — especially the uterus and the myoepithelial cells around milk ducts — that rise in intracellular calcium drives contraction. Oxytocin also promotes local prostaglandin production, which amplifies uterine contractility.
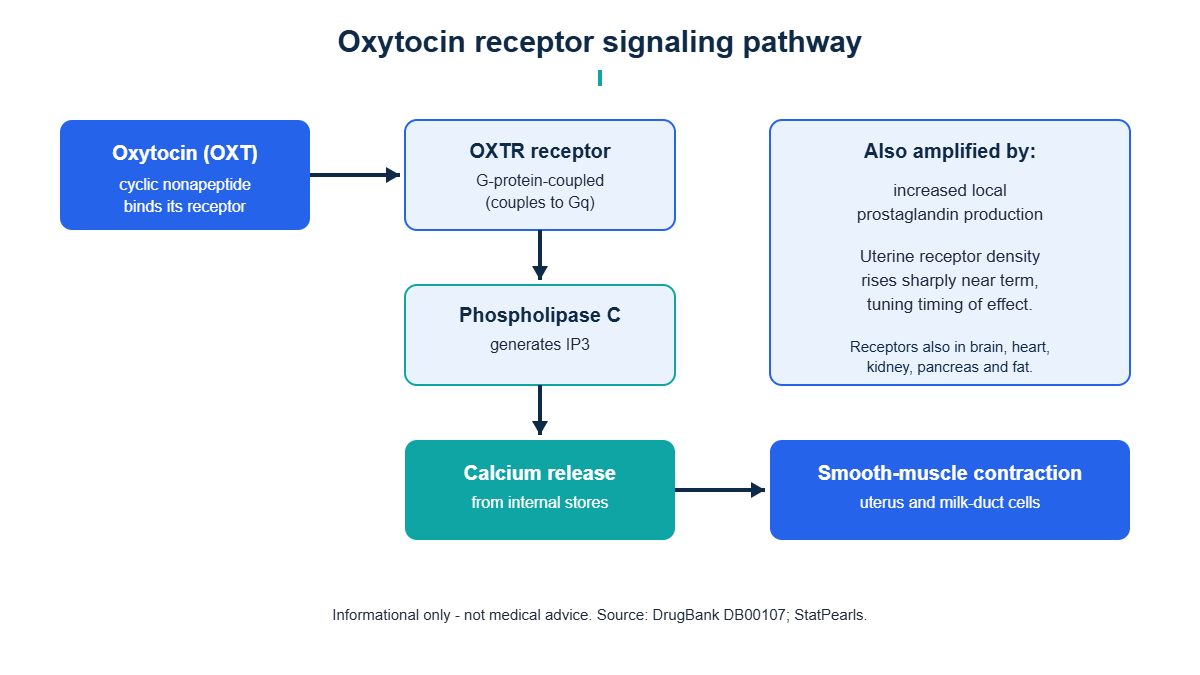
Receptor density is dynamic. Uterine oxytocin receptors increase dramatically toward the end of pregnancy, which helps explain why the same hormone has little effect early in pregnancy but a powerful effect at term. Outside reproduction, oxytocin receptors have been mapped in the brain, heart, kidney, thymus, pancreas, and fat tissue, and a great deal of research focuses on receptor populations in regions tied to social and emotional processing, such as the amygdala. Key features researchers point to include:
- A single primary receptor (OXTR) coupled mainly to Gq/phospholipase C and intracellular calcium signaling.
- Cross-reactivity with vasopressin receptors, owing to the close structural similarity of the two peptides.
- Up-regulation of uterine OXTR near term, linking receptor expression to physiological timing.
- Central oxytocin release within the brain (not just into blood), proposed to modulate social and stress circuitry.
- Variation in the OXTR gene, which is studied as a possible reason individual responses differ so widely.
Reported effects in the research literature
Oxytocin’s best-established effects are reproductive and physiological. In the behavioral and psychiatric literature, effects are reported but far more variable. Commonly described findings include:
- Uterine contraction during labor and after delivery (the basis of its FDA-approved clinical use).
- The milk-ejection (“let-down”) reflex during breastfeeding.
- In some studies, increased eye contact, attention to faces, and self-reported trust after intranasal dosing.
- Modulation of stress and anxiety responses in animal models, with less consistent human data.
- Roles in pair-bonding and parental behavior, much of it derived from animal research such as prairie vole studies.
What this does not mean: oxytocin is not a proven “love drug,” trust booster, or treatment for social difficulties. Many behavioral findings come from small, short studies, and several large, well-designed trials have failed to replicate early positive results. Effects appear to depend heavily on dose, context, baseline traits, and possibly genetics. The gap between dramatic animal results and modest, inconsistent human results is one of the central unresolved problems in the field.
What the human evidence shows
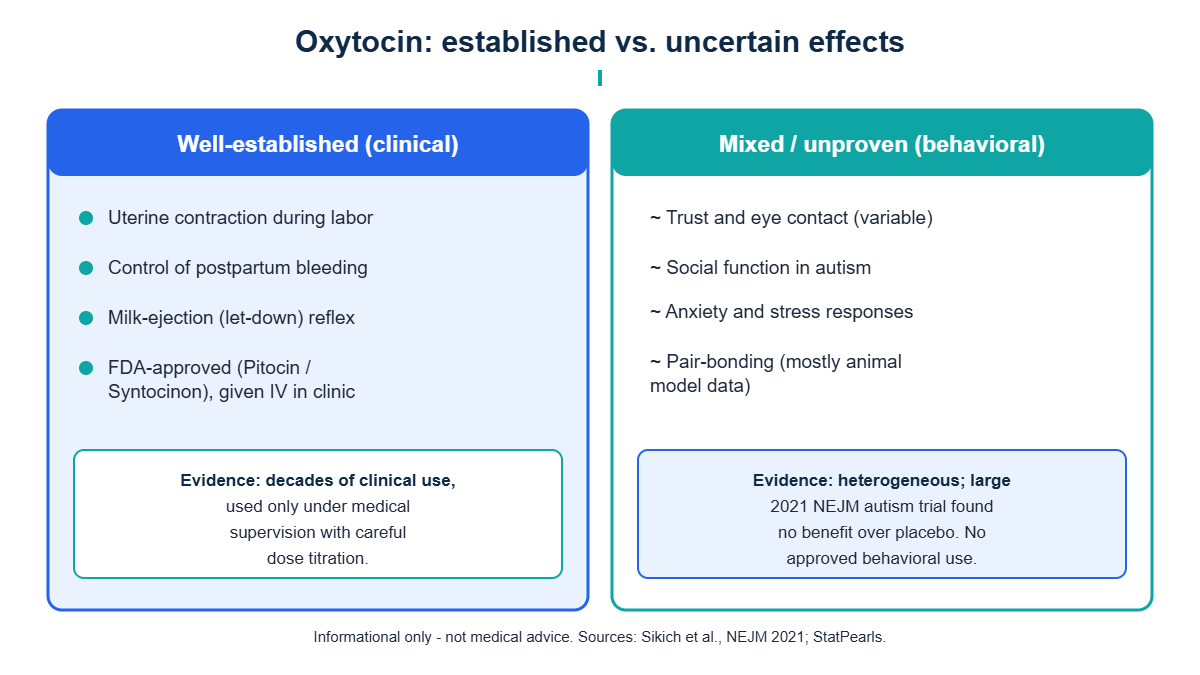
The strongest human evidence is in obstetrics. Synthetic oxytocin is FDA-approved and globally used for the medically supervised induction and augmentation of labor and for controlling postpartum hemorrhage. In that setting it is given intravenously, carefully titrated by clinicians, because over-stimulation of the uterus carries real risks. This use is decades old and well documented.
The behavioral evidence is much weaker. Intranasal oxytocin has been tested extensively in autism spectrum disorder, social anxiety, schizophrenia, and related conditions. The picture is mixed: some small trials and meta-analyses report modest benefits on social measures, while one of the largest and most rigorous studies — a multi-site randomized trial published in the New England Journal of Medicine in 2021 — found no significant benefit of intranasal oxytocin over placebo on social function in children and adolescents with autism. Reviews of the broader literature repeatedly conclude that results are heterogeneous and that no behavioral indication is considered an established, approved treatment. In short, oxytocin is a genuine approved drug for a narrow set of reproductive indications, and an actively investigated but unproven agent for everything else.
Handling, storage and reconstitution (research context)
Oxytocin is a small peptide whose disulfide bridge makes it sensitive to oxidation, heat, and trace metals. General laboratory handling principles for the lyophilized reference material include:
- Store lyophilized powder sealed, desiccated, and protected from light at -20 C or colder for long-term stability.
- Allow sealed vials to reach room temperature before opening to limit condensation and moisture uptake.
- Reconstitute gently with an appropriate sterile diluent, directing the stream against the vial wall rather than onto the powder; avoid vigorous shaking.
- Keep reconstituted solution refrigerated at 2-8 C, protected from light, and use within a short window.
- Avoid repeated freeze-thaw cycles of solution, which can degrade the peptide; trace-metal-free water and chelators help limit oxidative breakdown.
For step-by-step technique, see the linked reconstitution and sterile-technique resources below. This section describes general laboratory practice for reference material and is not instruction for human use.
Cautions and considerations
- Informational only — this page is not medical advice and does not endorse any human use of oxytocin outside licensed clinical care.
- Clinical oxytocin (e.g., Pitocin) is a prescription drug administered only under medical supervision; misuse, including uterine over-stimulation, can be dangerous.
- Because oxytocin overlaps with vasopressin receptors, high or prolonged exposure can affect fluid balance and, in clinical contexts, has been linked to water retention (hyponatremia).
- Behavioral effects are unproven; self-experimentation is not supported by reliable evidence and is outside the scope of this resource.
- Research-grade peptides are not approved for human consumption and should be handled only by qualified individuals in appropriate settings.
Frequently asked questions
Is oxytocin really the “love hormone”?
That nickname comes from its role in bonding, birth, and breastfeeding, and from animal studies on pair-bonding. But in humans the social effects are inconsistent and context-dependent, and many large trials have not confirmed the popular claims. It is more accurate to call it a reproductive hormone with proposed, still-debated social roles.
Is oxytocin FDA-approved?
Yes, but only in a specific form and use. Synthetic oxytocin (Pitocin, Syntocinon) is FDA-approved for inducing or augmenting labor and for controlling bleeding after childbirth. It is not approved for social, mood, or anti-aging purposes.
Why is oxytocin’s half-life so short?
As a small peptide, oxytocin is rapidly broken down by enzymes (including placental and plasma aminopeptidases), giving a plasma half-life on the order of just a few minutes. This is why clinical use relies on continuous intravenous infusion rather than a single dose.
How is oxytocin different from vasopressin?
The two hormones differ by only two of their nine amino acids and share an evolutionary origin, so they can cross-activate each other’s receptors. Vasopressin mainly controls water balance and blood pressure, while oxytocin is associated with reproduction and social behavior — but their structural overlap is why some of oxytocin’s side effects resemble vasopressin’s.
Related compounds and further reading
- How to reconstitute peptides
- Sterile technique
- Browse the full peptide library
- Reconstitution calculator
Share this article
References
- PubChem Compound Summary for CID 439302, Oxytocin. NIH/NLM 2026
- Oxytocin (DB00107): Uses, Interactions, Mechanism of Action. DrugBank Online 2026
- Osilla EV, Sharma S. Oxytocin. StatPearls. NCBI Bookshelf 2024
- Sikich L, et al. Intranasal Oxytocin in Children and Adolescents with Autism Spectrum Disorder. N Engl J Med 2021;385:1462-1473
- Jurek B, Neumann ID. The Oxytocin Receptor: From Intracellular Signaling to Behavior. Physiol Rev 2018;98(3):1805-1908
- Oxytocin. Wikipedia 2026
For informational use only. Not medical advice; consult a qualified healthcare professional. 21+.
Oxytocin reconstitution calculator
Use the calculator below to find the concentration (mg/mL), draw volume and U-100 syringe units for Oxytocin once it is reconstituted with bacteriostatic water. Oxytocin has molecular formula C43H66N12O12S2 and a molecular weight of 1007.19 g/mol. Enter your vial amount and the water volume to see the lab math — informational use only, not dosing advice.