Tesamorelin
Summary
Tesamorelin is a stabilized GHRH (GRF 1-44) analog, FDA-approved as EGRIFTA to reduce excess visceral abdominal fat in HIV-associated lipodystrophy by stimulating the body’s own growth hormone.
Quick facts
| Also known as | EGRIFTA, TH9507, GRF analog, tesamorelin acetate |
| Category | Growth hormone secretagogue / GHRH (GRF) analog |
| Status | FDA-approved (HIV-associated lipodystrophy) |
| CAS | 218949-48-5 |
| Formula | C221H366N72O67S |
| Molecular weight | ≈5135.9 g/mol |
| Sequence | Human GRF(1-44) with N-terminal trans-3-hexenoyl modification |
| Half-life | ≈26–38 minutes |
| Storage | Lyophilized: refrigerate, protect from light. Reconstituted: 2–8°C, do not freeze. |
In Plain English
Tesamorelin is a lab-made peptide that prompts the body to release its own growth hormone. It is an approved medicine used to reduce excess deep belly fat in certain patients. Researchers study it for body-fat and growth-hormone effects.
Tesamorelin is a stabilized synthetic analog of growth-hormone-releasing hormone (GHRH) and the only such peptide to earn full FDA approval. Marketed as EGRIFTA, tesamorelin was approved in 2010 to reduce excess visceral abdominal fat in people with HIV-associated lipodystrophy. Developed by Theratechnologies (originally coded TH9507), it is a 44-amino-acid GHRH (also called GRF) molecule protected against rapid breakdown by a chemical modification at its N-terminus.
What is tesamorelin?
Tesamorelin is built on the full 44-residue sequence of human growth-hormone-releasing factor (GRF 1-44). Native GHRH is degraded almost immediately in the bloodstream, so tesamorelin attaches a trans-3-hexenoyl group (a short six-carbon chain with a double bond) to the N-terminal tyrosine. This modification slows enzymatic degradation while preserving the molecule’s ability to activate the GHRH receptor. The result is a peptide with the molecular formula C221H366N72O67S and a molecular weight of about 5,136 g/mol (CAS 218949-48-5). Unlike injected growth hormone, tesamorelin does not supply GH directly — it prompts the pituitary gland to release the body’s own growth hormone in its natural, pulsatile rhythm.
How tesamorelin is studied to work
Tesamorelin acts upstream in the growth-hormone axis. By mimicking GHRH it stimulates the pituitary to secrete growth hormone, which in turn raises insulin-like growth factor 1 (IGF-1) from the liver. The key reported pathways are:
- GHRH receptor binding: activates GHRH receptors on pituitary somatotroph cells.
- Pulsatile GH release: increases secretion of the body’s own growth hormone while preserving normal feedback control.
- IGF-1 elevation: downstream rise in IGF-1, the mediator of many GH effects.
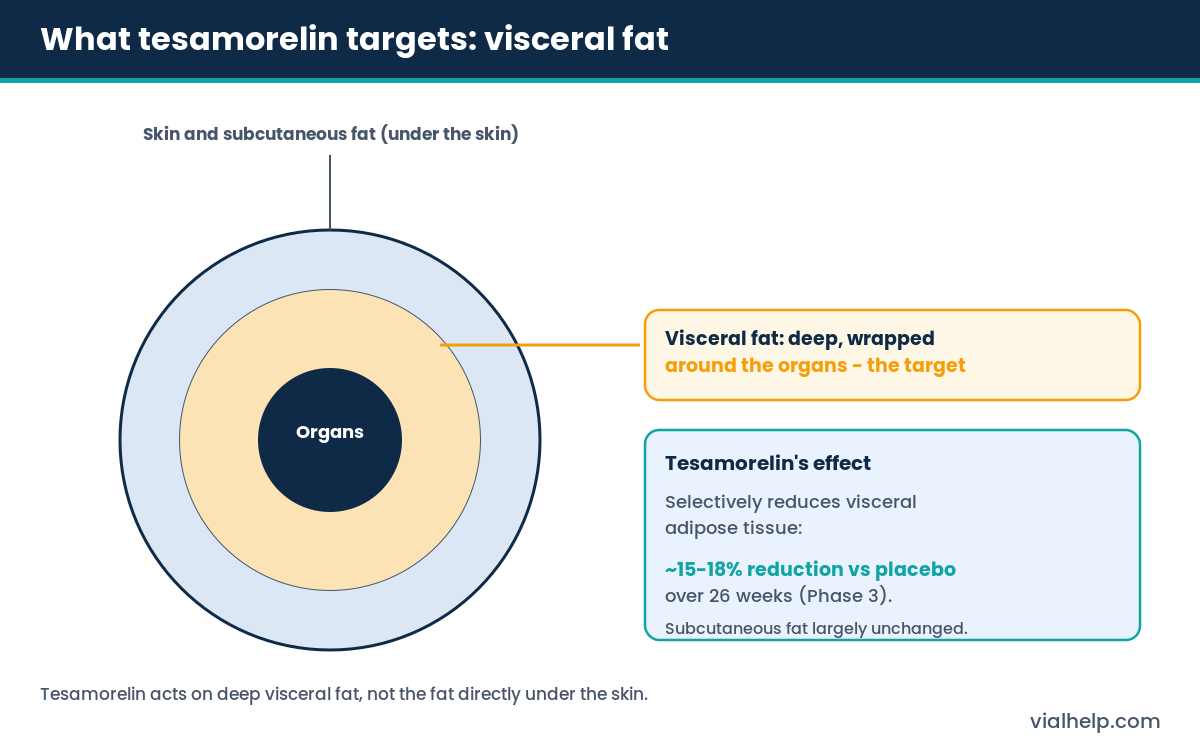
- Lipolysis: growth hormone promotes breakdown of visceral (deep abdominal) fat, the basis of its approved indication.
Reported effects and benefits in the research literature
The clinical literature on tesamorelin, much of it in people with HIV-associated lipodystrophy, reports:
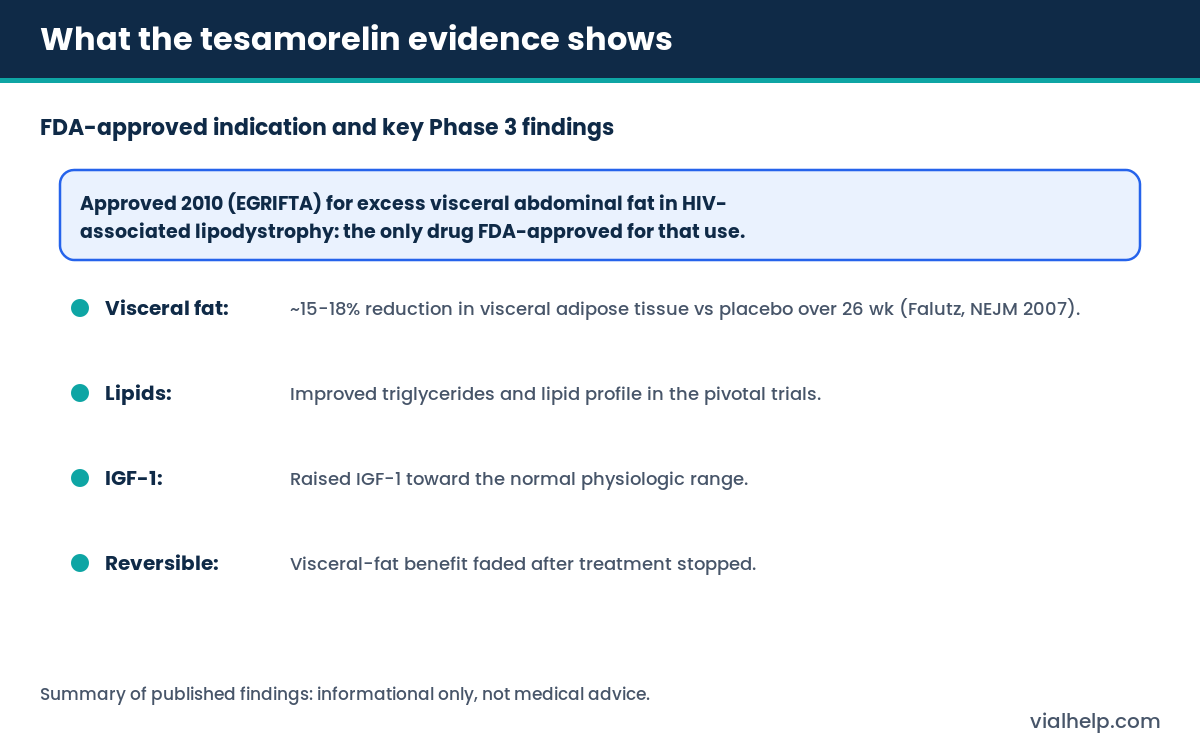
- Reduced visceral fat — roughly a 15–18% reduction in visceral adipose tissue versus placebo over 26 weeks in the pivotal Phase 3 trials.
- Improved lipids — lower triglycerides and improvements in the overall lipid profile.
- Higher IGF-1 — IGF-1 raised toward the normal physiologic range.
- Studied in liver fat — later research examined tesamorelin’s effect on liver fat (NAFLD) in people with HIV.
What this does not mean: the visceral-fat benefit was specific to a defined patient population and reversed after treatment stopped. These findings do not establish tesamorelin as a general fat-loss or anti-aging agent, and it carries cautions around blood sugar and fluid retention.
What the human evidence shows
Tesamorelin has a strong human evidence base. The landmark Phase 3 trial by Falutz and colleagues (New England Journal of Medicine, 2007) showed a selective reduction in visceral abdominal fat with simultaneous lipid improvements over six months, leading to FDA approval of EGRIFTA in 2010 for HIV-associated lipodystrophy — still the only drug approved for that specific use. Newer formulations (EGRIFTA SV and EGRIFTA WR) have since been approved with bioequivalence data. Reported adverse effects include injection-site reactions, joint pain, fluid retention and increases in blood glucose, reflecting the expected effects of raising growth hormone. Outside the HIV-lipodystrophy indication, tesamorelin remains investigational.
Handling, storage and reconstitution (research context)
- Lyophilized: keep refrigerated and protected from light until reconstitution; GHRH peptides are sensitive to heat and moisture.
- Reconstituted: refrigerate at 2–8°C, use within the window indicated by the supplier’s certificate of analysis, and avoid freezing or vigorous shaking.
- Convert vial mg and diluent volume to a clear mg/mL value with the reconstitution calculator.
- Remember that syringe “units” are a volume marking, not a dose — see IU vs mL.
Cautions and considerations
- Tesamorelin sold as a research peptide is not the FDA-approved finished product (EGRIFTA) and is not quality-assured for human use.
- Because it raises growth hormone and IGF-1, it carries the same theoretical cautions as GH therapy (glucose, fluid balance).
- Confirm purity, identity and endotoxin against a current COA — see our COA guide.
- This page is informational only and is not medical advice; consult a qualified healthcare professional.
Frequently asked questions
Is tesamorelin the same as growth hormone?
No. Tesamorelin is a GHRH analog that stimulates the pituitary to release the body’s own growth hormone, rather than supplying growth hormone directly.
What is tesamorelin FDA-approved for?
It is approved (as EGRIFTA) to reduce excess visceral abdominal fat in adults with HIV-associated lipodystrophy — the only approved indication.
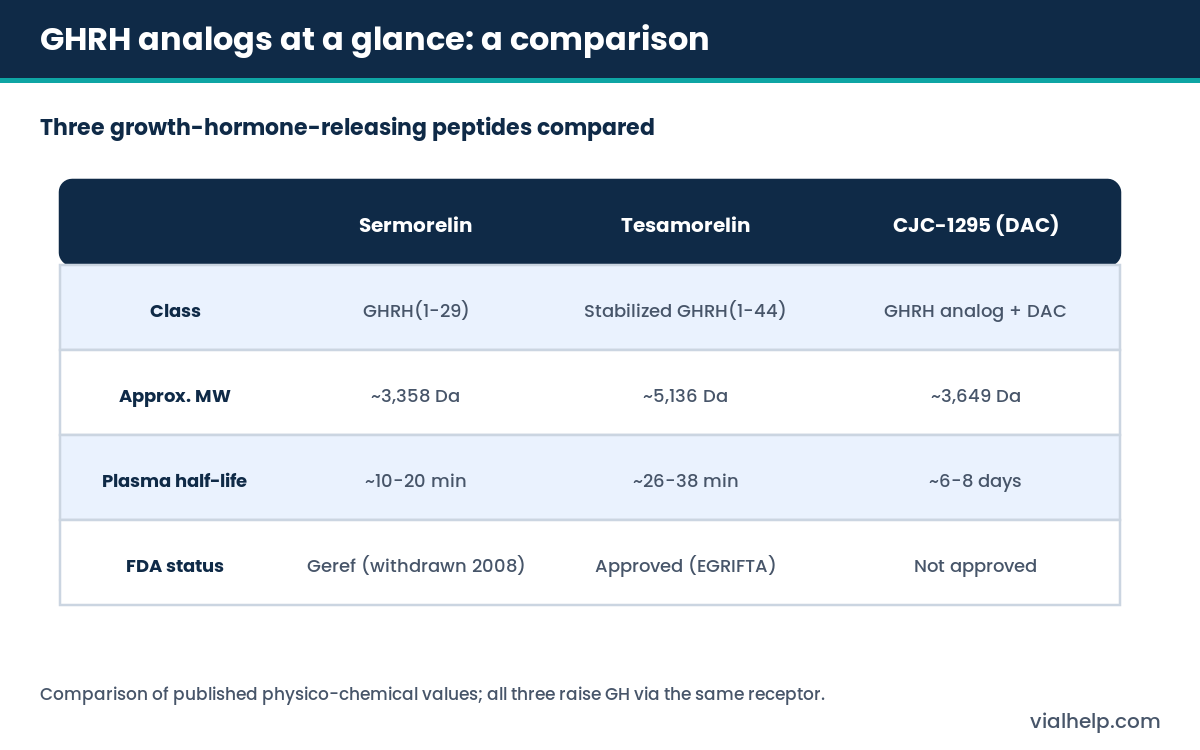
How is tesamorelin different from sermorelin and CJC-1295?
All three are GHRH-based. Sermorelin is the short GRF(1-29) fragment, tesamorelin is a stabilized full-length GRF(1-44) with a longer half-life, and CJC-1295 with DAC binds albumin for a multi-day half-life. See the comparison below.
Why is tesamorelin’s effect on fat reversible?
The visceral-fat reduction depends on continued GH stimulation; in trials the benefit faded once treatment was discontinued.
Related compounds and further reading
- CJC-1295 (with DAC) — a long-acting GHRH analog in the same family.
- Sermorelin — the GRF(1-29) GHRH fragment.
- Ipamorelin — a GH secretagogue often discussed alongside GHRH analogs.
- Browse the full peptide library and our research guides; background on measurement in IU vs mL.
- How to reconstitute peptides — step-by-step reconstitution method and concentration math.
- Sterile technique — aseptic handling and contamination prevention for research vials.
Share this article
References
For informational use only. Not medical advice; consult a qualified healthcare professional. 21+.
Tesamorelin reconstitution calculator
Use the calculator below to find the concentration (mg/mL), draw volume and U-100 syringe units for Tesamorelin once it is reconstituted with bacteriostatic water. Tesamorelin has molecular formula C221H366N72O67S and a molecular weight of ≈5135.9 g/mol. Enter your vial amount and the water volume to see the lab math — informational use only, not dosing advice.