GLP-1 Side Effects: Semaglutide and Tirzepatide Explained
Informational guide
GLP-1 side effects are, for most people, a story about the gut. Drugs in this class — including semaglutide and the dual GIP/GLP-1 agonist tirzepatide — share a recognizable profile of mostly mild-to-moderate gastrointestinal effects that tend to be worst early and ease over time. This article explains what the research literature reports, why these effects happen, and how studies and product labels describe managing them.
Why GLP-1 drugs cause side effects in the first place
GLP-1 receptor agonists imitate an incretin hormone the gut releases after eating. Two of their core actions — slowing how fast the stomach empties and signaling fullness to the brain — are exactly the mechanisms that also produce the most common complaints. Slower gastric emptying can feel like nausea, early fullness or reflux; the appetite-suppressing signal can blunt interest in food to the point of under-eating. Tirzepatide adds GIP-receptor activity on top of GLP-1, and in clinical-development data it has shown a broadly similar but sometimes more pronounced gastrointestinal profile.
The most commonly reported GLP-1 side effects
Across the SURPASS (diabetes) and SURMOUNT (obesity) programs, the gastrointestinal effects below are the ones reported most often. Rates depend heavily on dose and how quickly the dose is escalated.
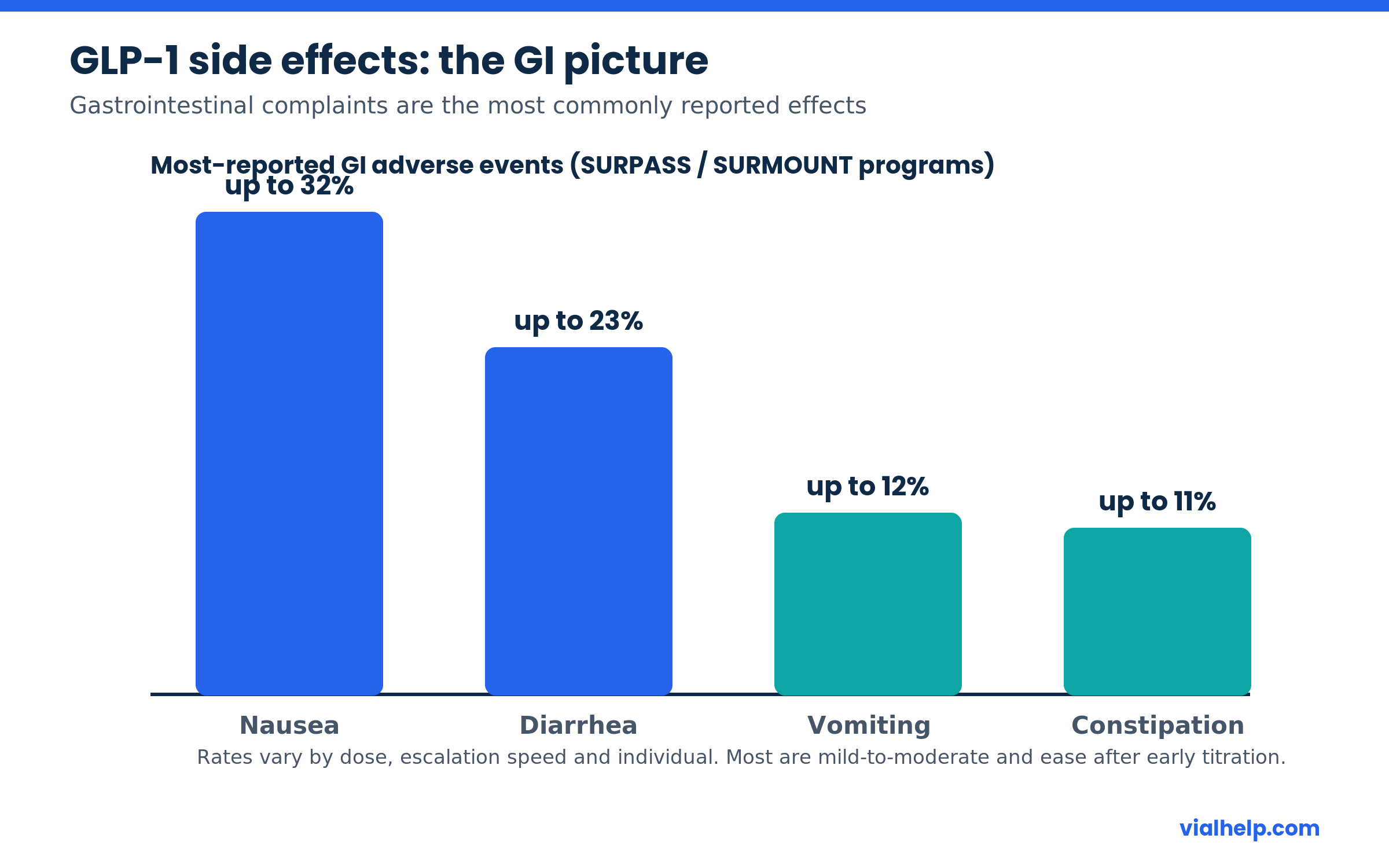
- Nausea — the single most common effect, reported in up to roughly a third of participants at higher doses.
- Diarrhea — frequent, often overlapping with the early titration period.
- Vomiting — less common than nausea but a notable reason for dose adjustment.
- Constipation — reflects slowed gut transit; usually managed with fluids and fiber.
- Reduced appetite and early fullness — intended effects that can tip into under-eating.
Why side effects usually ease over time
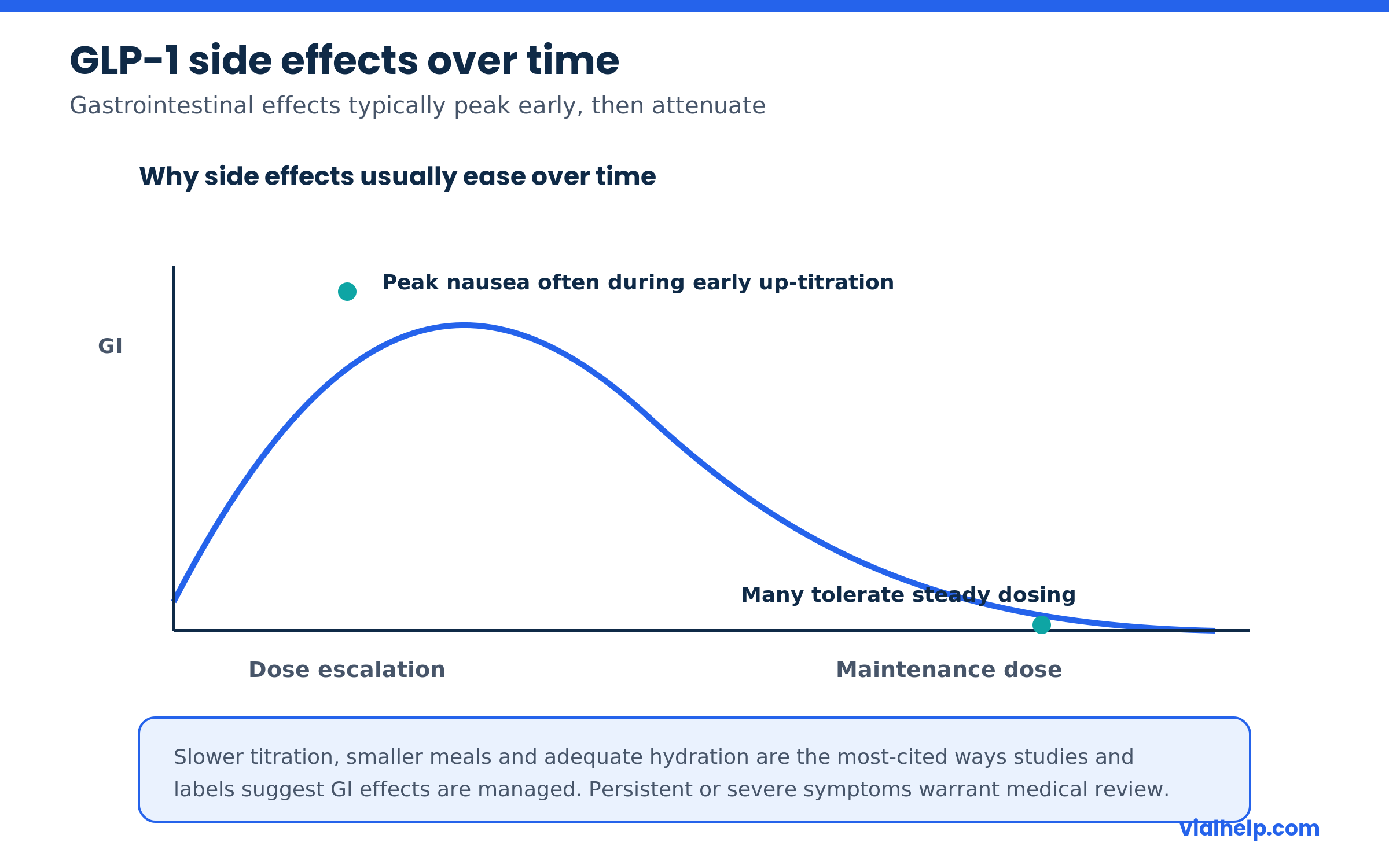
One of the most consistent findings is that gastrointestinal intolerance is generally worst during early dose escalation and attenuates as the body adapts to a steady dose. This is the rationale behind the slow, stepwise titration schedules used in trials and on approved labels: starting low and increasing gradually gives the gut time to adjust and reduces the peak intensity of nausea.
Less common but more serious considerations
Beyond everyday GI complaints, product labels and the published literature flag a number of less frequent but more important issues that are reasons to involve a clinician:
- Pancreatitis — rare but reported; severe, persistent abdominal pain warrants prompt medical attention.
- Gallbladder problems — rapid weight loss of any kind is associated with gallstones.
- Dehydration and kidney strain — secondary to prolonged vomiting or diarrhea.
- Thyroid C-cell tumor signal — seen in rodents; the human relevance is uncertain, but these drugs carry a boxed warning and are contraindicated with a personal or family history of medullary thyroid carcinoma or MEN 2.
- Hypoglycemia — low on their own, but higher when combined with insulin or sulfonylureas.
What about side effects beyond the GI tract?
Other commonly mentioned effects include injection-site reactions, fatigue and headache, particularly during the adjustment period. There is also active discussion about loss of lean muscle mass alongside fat during rapid weight loss, which is why adequate protein and resistance activity are frequently raised in the literature. None of this is a substitute for individualized medical guidance.
How tolerability is managed in the research and clinical record
- Use the slow, stepwise dose-escalation schedule rather than jumping to a high dose.
- Smaller, lower-fat meals and stopping at the first sign of fullness reduce nausea.
- Maintaining hydration offsets fluid loss from diarrhea or vomiting.
- Persistent, severe, or alarming symptoms (intense abdominal pain, repeated vomiting) are reasons to seek medical care, not to push through.
Frequently asked questions
Do semaglutide and tirzepatide have the same side effects?
Their profiles are similar — both are dominated by gastrointestinal effects — but comparative analyses suggest tirzepatide can carry a somewhat higher rate of nausea and diarrhea, likely reflecting its added potency and GIP activity.
How long do GLP-1 side effects last?
For most people the worst nausea is concentrated in the early dose-escalation weeks and eases at a steady maintenance dose, though individual variation is wide.
Are GLP-1 side effects a reason to stop the drug?
Mild GI effects often settle with time and titration adjustments. Severe or persistent symptoms, or any warning signs of pancreatitis or gallbladder disease, should be evaluated by a healthcare professional.
Does eating differently help?
The literature consistently points to smaller, lower-fat meals, eating slowly, and stopping when full as practical ways to limit nausea.
References
US Pharmacist — GI Adverse Effects of GLP-1 Receptor Agonists: link
Jastreboff AM et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1), NEJM 2022: link
Wilding JPH et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1), NEJM 2021: link
Comparative GI adverse effects of GLP-1 receptor agonists, network meta-analysis (PMC): link
Informational only — not medical advice. This article summarizes published research and product labeling and does not recommend any specific product, brand, or personal dosing. Consult a qualified healthcare professional before making decisions about any medication. 21+.