Subcutaneous vs Intramuscular Injection: SubQ vs IM Explained
HANDLING & TECHNIQUE
Subcutaneous vs intramuscular injection is one of the most common questions in peptide handling, and the difference comes down to how deep the needle goes. A subcutaneous (SubQ) injection places material in the fat layer just under the skin, while an intramuscular (IM) injection goes deeper into the muscle. That single difference drives everything else: the needle you use, the angle, how much you can inject, and how fast it is absorbed.
Subcutaneous vs intramuscular injection: what is the difference?
Every injection has to cross the same outer barrier of skin, but the two routes stop at different depths. A subcutaneous injection deposits fluid into the loose fatty tissue (the hypodermis) that sits below the dermis and above muscle. An intramuscular injection passes through the skin and fat and delivers the fluid into the muscle belly itself. Because muscle carries a much richer blood supply than fat, the route you choose changes how quickly the body picks the substance up and how much you can comfortably give at once.
Skin and tissue layers: where each injection goes
Understanding the layers makes the technique intuitive. From the surface down, the skin has the epidermis (a thin outer barrier, roughly 0.06 to 0.6 mm), the dermis (about 1 to 4 mm of connective tissue full of nerves and small vessels), the subcutaneous fat (the hypodermis, anywhere from about 5 to 20 mm thick and highly variable between people and sites), and then the muscle beneath it. A SubQ needle only needs to reach the fat; an IM needle has to clear the fat and enter the muscle, which is why body size and fat thickness change the needle length that is appropriate.
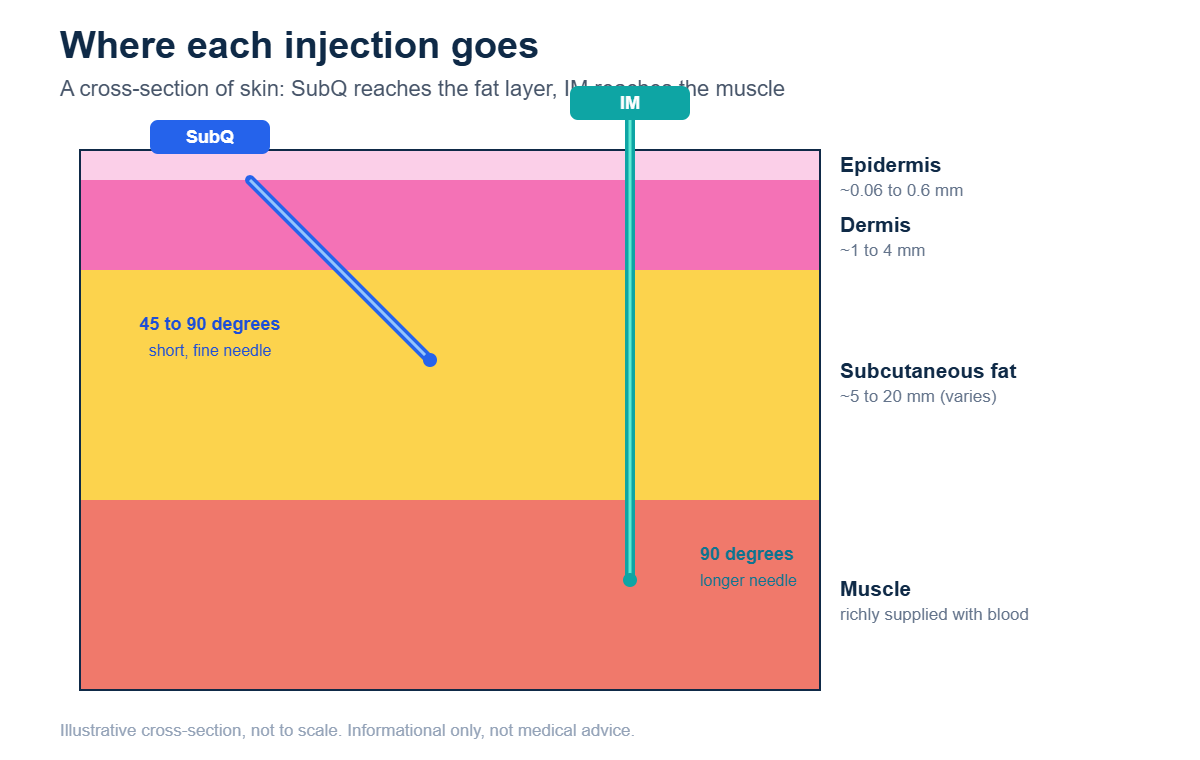
Subcutaneous (SubQ) injections: angle, needle size, sites and absorption
SubQ is the gentler, more forgiving route and the one most people can perform themselves.
- Angle: 90 degrees for average or heavier tissue, or 45 degrees while pinching a fold of skin when the fat layer is thin, to avoid reaching muscle.
- Needle length: short, commonly about 4 to 16 mm (pen and insulin needles are shortest; a 1/2 inch needle is typical).
- Gauge: fine, generally 25 to 31G. Insulin syringes are usually 29 to 31G, which is why SubQ injections tend to sting less.
- Common sites: the abdomen (avoiding a roughly two-inch circle around the navel), the front or outer thigh, and the back of the upper arm.
- Volume: small, generally about 1 to 1.5 mL; larger volumes in fat cause more pressure and discomfort.
- Absorption: slower and more sustained, because fat is poorly vascularized. This gives a lower, flatter peak, a depot-like release that suits many peptides.
Intramuscular (IM) injections: angle, needle size, sites and absorption
IM reaches a deeper, blood-rich compartment and is used when a product needs more volume or a different absorption profile.
- Angle: 90 degrees, straight in, so the needle clears the fat and enters muscle.
- Needle length: longer, commonly 1 to 1.5 inches (about 25 to 38 mm), chosen for body size so it actually reaches muscle.
- Gauge: wider bore, roughly 20 to 25G; thick, oil-based solutions often need an even larger bore (about 18 to 21G) to draw and inject.
- Common sites: the deltoid (upper arm), the vastus lateralis (outer thigh), and the ventrogluteal site (hip), which is often considered the safest large-muscle option.
- Volume: more than SubQ, up to roughly 2 mL in the deltoid and 2 to 3 mL in larger muscles.
- Absorption: faster for water-based drugs because muscle is well supplied with blood, giving a higher peak; oil-based esters instead form a slow depot that releases over days to weeks.
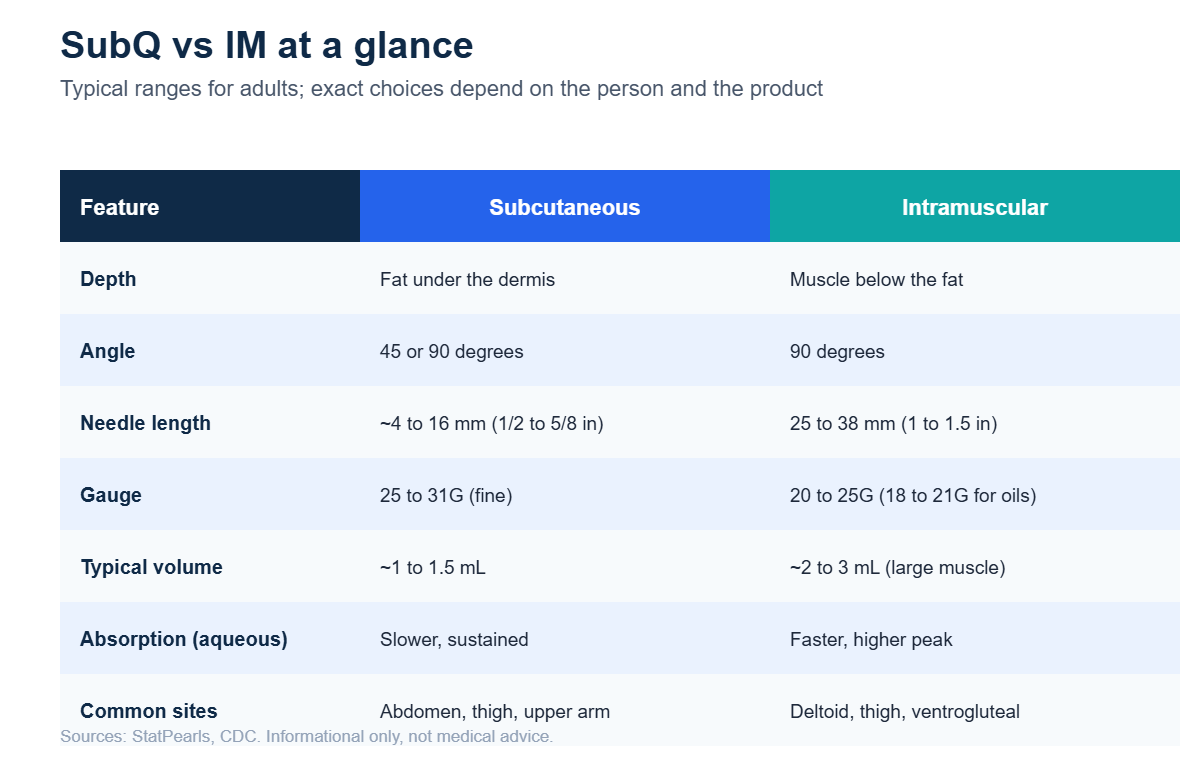
SubQ vs IM at a glance
The table below summarizes the typical adult ranges. Treat them as general reference points, not fixed rules, the right choice depends on the person, the site, and the specific product.
Why most research peptides and GLP-1s are subcutaneous
The majority of research peptides are supplied as small, water-based volumes after reconstitution, and that profile fits the subcutaneous route almost perfectly, small doses, a fine needle, and a slow, steady release. The best-known examples are the GLP-1 receptor agonists: semaglutide and tirzepatide are both labeled for subcutaneous use, rotated among the abdomen, thigh, and upper arm. Growth-hormone secretagogues and most healing and recovery peptides studied in the community are likewise handled subcutaneously.
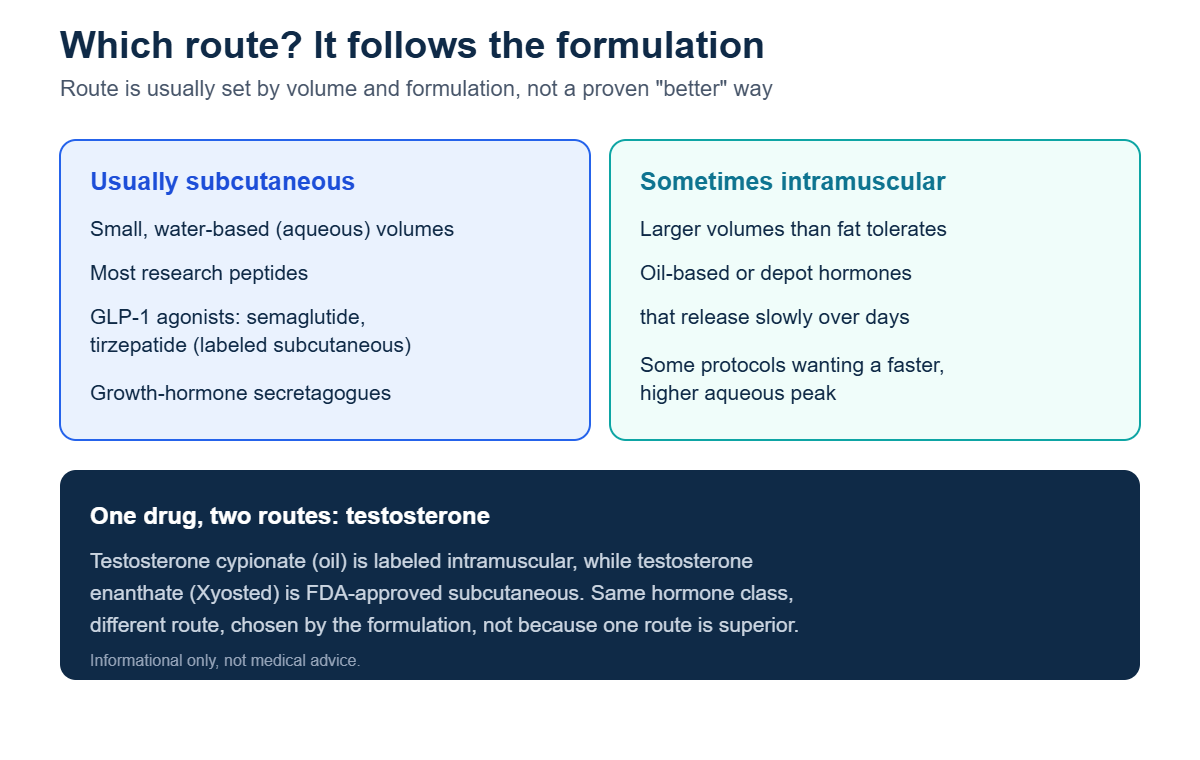
When intramuscular is used
Intramuscular delivery earns its place when the formulation calls for it. Larger volumes than fat can comfortably hold, thick oil-based or depot hormones designed to release slowly, and protocols that want a faster aqueous peak are the usual reasons. A clean, real-world illustration is testosterone: testosterone cypionate, an oil, is labeled intramuscular, whereas testosterone enanthate (as Xyosted) is FDA-approved for subcutaneous use. Same hormone class, two different routes, decided by the formulation rather than by one route being inherently better.
What the evidence does and does not show about route
It is tempting to assume one route is simply superior, but for most peptides the honest answer is that route is driven by formulation, volume, and the protocol that was actually studied, not by proven head-to-head superiority. Rigorous comparisons are limited. Some community practices, such as injecting BPC-157 or TB-500 close to an area of interest in the hope of a localized effect, are based on animal signals and anecdote rather than controlled human trials, there are no published randomized controlled human studies of BPC-157, and its optimal route in people is unknown. Where a manufacturer specifies a route, that instruction reflects how the product was tested and should be treated as the reference point.
Frequently asked questions
Are peptides subcutaneous or intramuscular?
Most research peptides and GLP-1 receptor agonists are subcutaneous, because they are small water-based volumes. Intramuscular is generally reserved for larger volumes or oil-based, slow-release formulations.
What size needle is used for SubQ versus IM?
SubQ typically uses a short, fine needle (about 4 to 16 mm, 25 to 31G). IM uses a longer, wider needle (about 25 to 38 mm, 20 to 25G, or a larger bore for oils).
Why does IM absorb faster than SubQ?
Muscle has a much richer blood supply than fat, so water-based drugs enter the bloodstream more quickly and reach a higher peak. Fat releases more slowly and steadily.
Can the same drug be given either way?
Sometimes, but usually only if a formulation exists for that route. The testosterone example shows how the same hormone is intramuscular in one form and subcutaneous in another.
References
- StatPearls — Intramuscular Injection. NCBI Bookshelf NBK556121
- StatPearls — Anatomy, Skin (Integument). NCBI Bookshelf NBK441980
- CDC — Vaccine Administration (Pink Book, Chapter 6). cdc.gov
- WHO — Best Practices for Injections and Related Procedures Toolkit. NCBI Bookshelf NBK138495
- FDA — Ozempic (semaglutide) Prescribing Information. accessdata.fda.gov
- FDA — Mounjaro (tirzepatide) Prescribing Information. accessdata.fda.gov
- USADA — BPC-157: Experimental Peptide Creates Risk for Athletes. usada.org
Informational only — not medical advice · 21+. This article explains general injection technique for educational and research context. It is not a personal dosing or self-injection protocol. Consult a qualified healthcare professional before making health decisions.