503A vs 503B compounding: what the difference means for peptides
“503A” and “503B” come up constantly in peptide regulation news, but the two terms describe very different things. Here is a clear, non-legal explainer of the two compounding pathways and why the distinction keeps appearing in peptide headlines.
Two different compounding pathways
Both 503A and 503B refer to sections of the Federal Food, Drug, and Cosmetic Act that describe how drugs may be compounded — that is, prepared outside of large-scale manufacturing. The simplest way to think about it: 503A is about traditional, prescription-based pharmacy compounding for a specific patient, while 503B is about FDA-registered “outsourcing facilities” that can make larger batches under stricter manufacturing oversight.
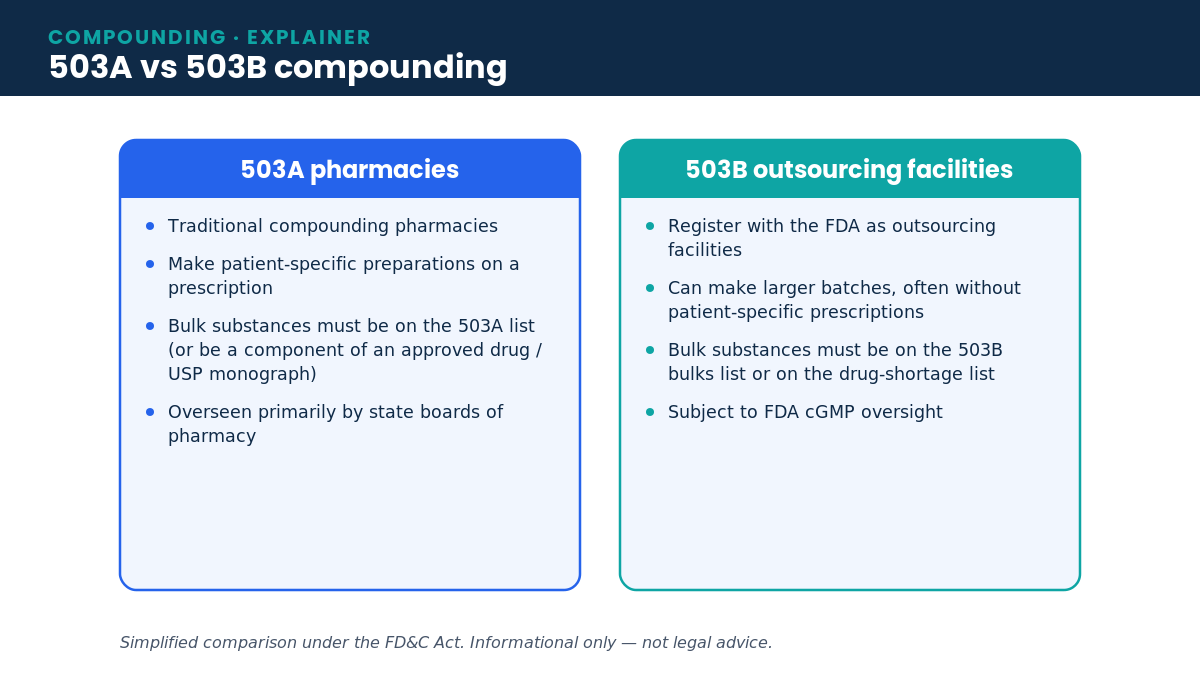
503A pharmacies generally compound in response to an individual prescription and are overseen primarily by state boards of pharmacy. 503B outsourcing facilities register with the FDA, can produce larger quantities (sometimes without a patient-specific prescription), and are subject to current Good Manufacturing Practice (cGMP) requirements and FDA inspection.
The role of the “bulk substances list”
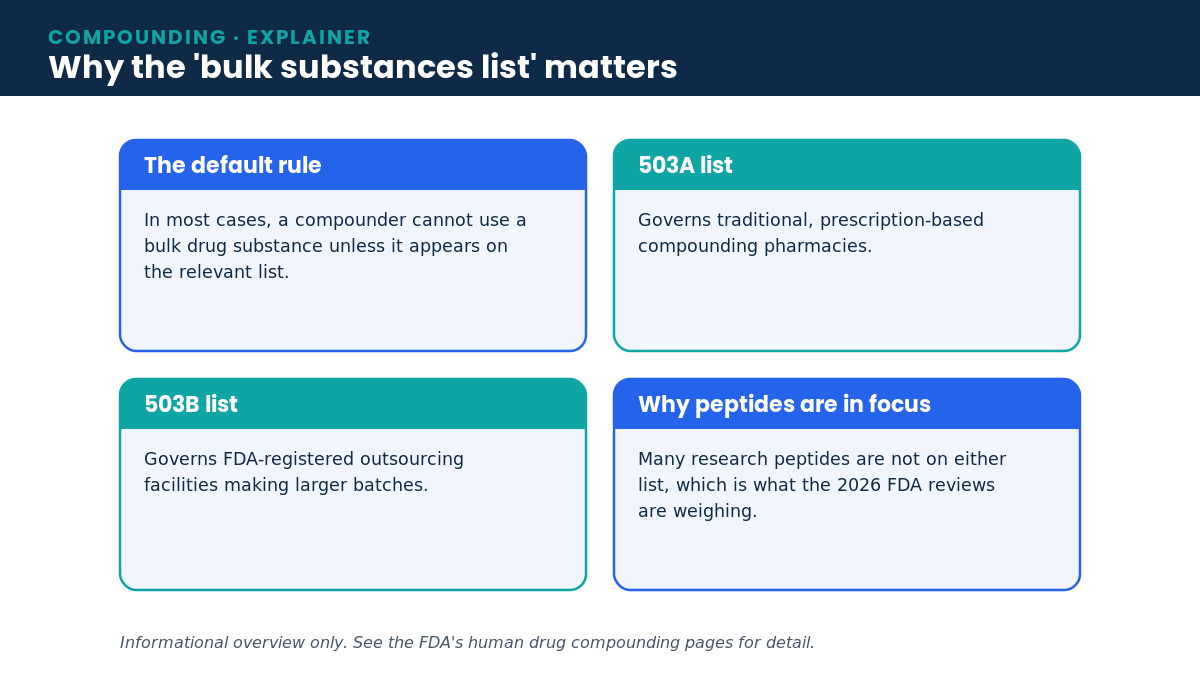
A recurring phrase in this area is the “bulk drug substances list.” In most cases, a compounder cannot use a raw bulk drug substance unless that substance is on the relevant list — the 503A list for traditional pharmacies, or the 503B list for outsourcing facilities. (There are narrow exceptions, such as substances that are components of an FDA-approved drug or that have a USP monograph.)
Where peptides fit
Many research peptides are not currently on either list. That is exactly why recent FDA activity has drawn so much attention: a July 2026 Pharmacy Compounding Advisory Committee meeting is weighing whether several peptides should be eligible under 503A, while separately the FDA has proposed excluding certain GLP-1 drugs (semaglutide, tirzepatide, liraglutide) from the 503B bulks list. These are distinct decisions on distinct lists, which is why it is easy to conflate them.
Why the distinction matters now
Following peptide regulation without separating 503A from 503B leads to confusion — a development on one list does not automatically apply to the other. Keeping the two pathways straight makes the news easier to interpret: 503A activity is about traditional compounding eligibility, while 503B activity is about outsourcing-facility manufacturing. Neither is a statement that a given peptide is an FDA-approved medicine.
Frequently asked questions
Is 503B “stronger” approval than 503A?
Neither is drug approval. 503B facilities face cGMP manufacturing oversight and can make larger batches; 503A is patient-specific compounding. They are different regulatory categories, not tiers of approval.
Does being on a bulk list mean a peptide is proven safe and effective?
No. Listing concerns eligibility for compounding, not the FDA’s safety-and-efficacy approval standard for finished drug products.
Related on VialHelp
See our explainer on the latest peptide regulatory news, the peptide library, and our guide to reading a Certificate of Analysis.
Sources: FDA — Human Drug Compounding laws and policies; FDA — 503B bulk drug substances; FDA — 503B GLP-1 exclusion proposal.
Share this article
For informational and educational use only — not medical or legal advice. Intended for adults 21+.