TRT (Testosterone) Side Effects: What the Evidence Shows
Side-effects series · Hormone therapy
Testosterone replacement therapy (TRT) is widely discussed alongside research peptides, so this entry in our side-effects series covers what the evidence shows about its risks. One framing note up front: testosterone is a steroid hormone, not a peptide — it appears here only as a closely related hormone-therapy topic. Everything below is informational and is not medical advice.
What TRT is
Testosterone replacement therapy restores testosterone in men diagnosed with hypogonadism — a clinical condition requiring both consistent symptoms and repeatedly, unequivocally low morning testosterone. The Endocrine Society and the American Urological Association both stress that diagnosis, not symptoms alone, drives treatment. The FDA notes testosterone is approved for hypogonadism due to specific medical conditions and that benefit and safety are not established for low testosterone from aging alone. Common approved formulations include injections, transdermal gels and patches, and implanted pellets.
Common, well-documented side effects
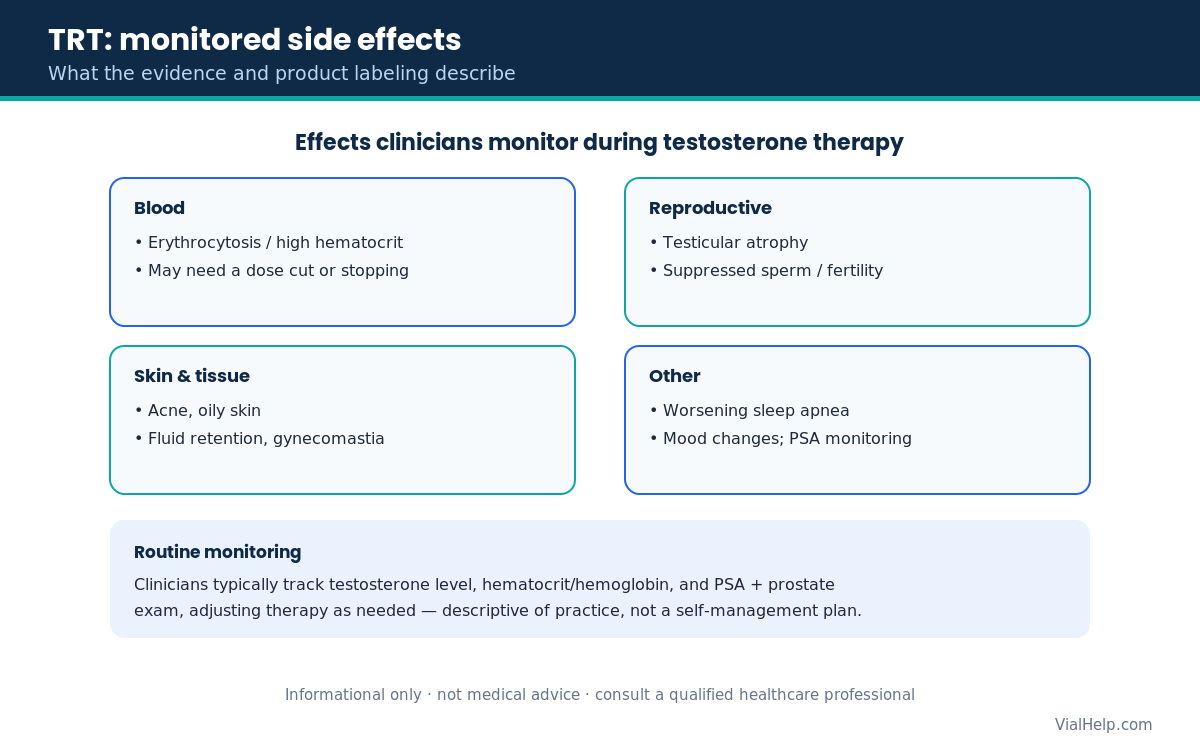
The following clusters are supported by FDA testosterone product labeling and the Endocrine Society guideline:
- Erythrocytosis (elevated hematocrit) — among the most consistent effects; rising red-cell counts may require lowering or stopping therapy, which is why blood counts are monitored.
- Acne and oily skin.
- Fluid retention / edema — clinically important in men with heart, kidney, or liver disease.
- Gynecomastia — partly from testosterone converting to estradiol.
- Testicular atrophy and reduced fertility — exogenous testosterone suppresses the hypothalamic-pituitary-gonadal axis, lowering the signals that drive sperm production.
- Injection-site or skin reactions — gels carry a warning about secondary transfer to women and children through skin contact.
- Worsening obstructive sleep apnea, particularly with existing risk factors.
- Mood or behavioral changes — more pronounced at supraphysiologic (abused) doses.
Cardiovascular and prostate considerations
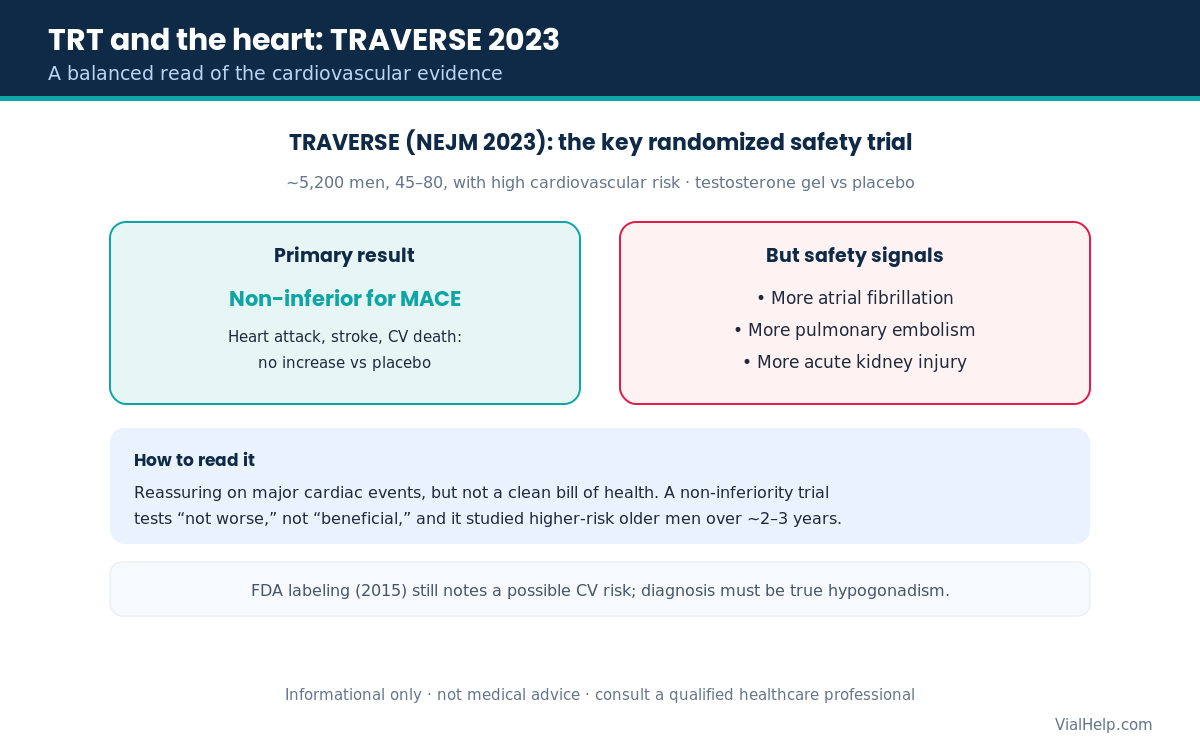
In 2015 the FDA required class-wide labeling changes adding language about a possible increased risk of heart attack and stroke, and clarifying that testosterone is not approved for age-related low testosterone. The picture became clearer with the 2023 TRAVERSE trial — a randomized, placebo-controlled study of roughly 5,200 men aged 45–80 with high cardiovascular risk. Testosterone was non-inferior to placebo for major adverse cardiac events (heart attack, stroke, cardiovascular death). However, the testosterone group showed more atrial fibrillation, pulmonary embolism, and acute kidney injury — real signals that should be weighed alongside the reassuring primary result.
For the prostate, guidelines call for baseline assessment and PSA monitoring. Current evidence does not show that properly monitored TRT causes prostate cancer, but active prostate cancer is a contraindication, and some men experience worsening benign prostatic / urinary symptoms (the evidence on magnitude is mixed).
What clinicians monitor
Per the Endocrine Society, AUA, and FDA labeling, clinicians typically track serum testosterone (aiming for a mid-normal range), hematocrit/hemoglobin (for erythrocytosis), and PSA plus a prostate exam in age-appropriate men, adjusting therapy as needed. This describes clinical practice; it is not a self-management plan.
Who should be cautious or avoid TRT
- Men with active prostate or breast cancer (contraindicated).
- Men currently seeking fertility — guidelines recommend against starting TRT.
- Untreated severe sleep apnea, uncontrolled heart failure, or high thrombotic risk.
- Men with an elevated baseline hematocrit.
- Women, and anyone who is or could become pregnant (testosterone is contraindicated in pregnancy; avoid skin transfer from gels).
Frequently asked questions
Does TRT cause heart attacks and strokes?
The 2023 TRAVERSE trial found testosterone was non-inferior to placebo for major cardiac events over about 2–3 years in higher-risk men — it did not show an increase in those events. The same trial did see more atrial fibrillation, pulmonary embolism, and acute kidney injury, and 2015 FDA labeling still notes a possible cardiovascular risk. Reassuring on major events, but not a clean bill of health.
Can TRT affect fertility?
Yes. Testosterone from outside the body suppresses the signals that drive sperm production and can shrink the testes, reducing fertility. Guidelines advise against starting TRT in men who want to conceive. Effects are often, but not always, reversible after stopping.
Why are blood counts checked on TRT?
Testosterone can raise red-blood-cell mass (erythrocytosis), which thickens the blood. Labeling directs checking hematocrit before and during therapy; a high value may prompt a dose reduction or stopping.
Is “low T from aging” an approved reason for TRT?
No. The FDA states benefit and safety are not established for low testosterone due to aging alone; approval is for hypogonadism caused by specific medical conditions.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2018. academic.oup.com
- Lincoff AM, Bhasin S, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). N Engl J Med 2023;389:107–117 (PMID 37326322). pubmed.ncbi.nlm.nih.gov
- FDA Drug Safety Communication / class-wide labeling change on testosterone (2015). fda.gov
- AndroGel (testosterone gel) FDA Prescribing Information. accessdata.fda.gov
- Testosterone: MedlinePlus Drug Information (NIH/NLM). medlineplus.gov
Informational only — not medical advice; consult a qualified healthcare professional · 21+